Do Organs Continue to Grow After Theyve Been Donated
![]() Open access peer-reviewed chapter
Open access peer-reviewed chapter
Organ Donation and Transplantation: "Life after Death"
Submitted: November 13th, 2017 Reviewed: April 3rd, 2018 Published: July 25th, 2018
DOI: 10.5772/intechopen.76962

IntechOpen Downloads
1,820
Total Chapter Downloads on intechopen.com
Abstract
Organ donation is defined as giving an organ or part of an organ to be transplanted into another person. Organ transplantation is the only option to save lives in patients affected by terminal organ failures and improve their quality of life. However, there is a disparity exists between the supply and demand of donated organs, leads to a loss of many lives. The number of organ transplantation have gradually increased in the last two decades and provide excellent results in children and young adults, and are challenging by the growing proportion of elderly transplant patients with co morbidity. The results of organ transplantation continue to improve, as a consequence of the innovations and the improvements in peri-operative management. This chapter describes organ donation and transplantation and its trends and challenges.
Keywords
- organ donation
- motivation
- psychosocial
*Address all correspondence to: kanmanijob@aims.amrita.edu
1. Introduction
Organ donation is defined as giving an organ or part of an organ to be transplanted into another person. Organ transplantation is the only option to save lives in patients affected by terminal organ failures and improve their quality of life. However, there is a disparity exists between the supply and demand of donated organs, leads to a loss of many lives. The number of organ transplantation have gradually increased in the last two decades and provide excellent results in children and young adults, and are challenging by the growing proportion of elderly transplant patients with co morbidity. The results of organ transplantation continue to improve, as a consequence of the innovations and the improvements in peri-operative management.
Organ transplantation currently depends on the availability of human organs. Their scarcity means that there is a waiting list of almost 63,000 in the European Union, and over 100,000 people in the United States according to the recent survey. The process of obtaining organs for donation and transplantation purely depends on the resources of health services and by health professionals' performance in potential donor identification and management tasks. However, in accordance with the current legislation it is mainly subjected to a personal or family decision, strongly mediated by psychosocial processes. Therefore, the need to analyze and intervene both in the practices of the professionals involved in the process of organ generation and in the attitudes of the general population need to stressed and addressed [1, 2, 3, 4, 5].
Advertisement
2. Organ transplantation and organ donation: an overview
Organ transplantation involves the surgical implantation of an organ or section of an organ into a person whose own organ is failing. The donor organ may come from both deceased individual as well as from a living donor. The patients psychological and behavior aspect as well their emotional response and mental health and adherence to medical regimen should be assessed before and after organ transplantation. The living donor's psychological response towards organ donation (most commonly for kidney and liver segment transplantation) is an important aspect to consider in the transplantation process.
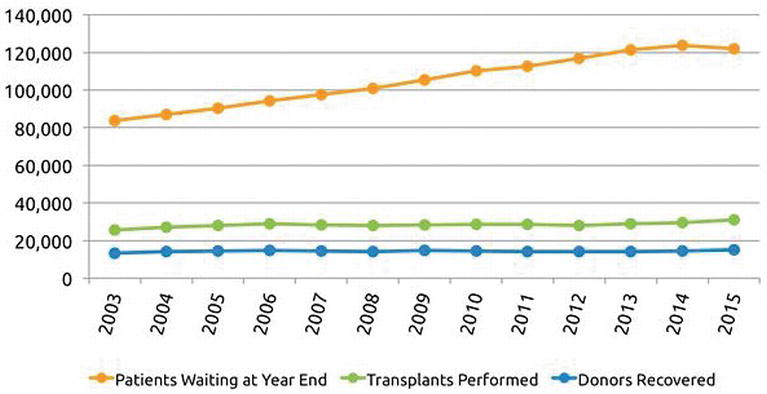
Organ donation is defined as "giving an organ or part of an organ to be transplanted into another person" (Organ procurement of Transplant Network (OPTN), 2015), organ donation has the potential to save lives. The organs donated from one single donor can save up to eight lives. Organ transplantation may be one of the options left to sustain someone's life. However, the disparity that exists between the supply and demand of donated organs, leads to a loss of many lives. Based on recent OPTN data, approximately 21 people will die each day while waiting for a transplant in the United States (US). Currently, 123, 358 people are awaiting organs and on the transplant list in the US with this number growing and the number of donated organs declining.
Asian Indians are more likely to have higher rates of having obesity and diabetes when compared with other Asian subgroups which make them at an increased risk of needing a donated organ [35]. These conditions can lead one to develop coronary artery disease and hypertension which then can lead to chronic kidney disease and other chronic illnesses. Patients who suffer from chronic kidney disease need regular dialysis which can ultimately lead them to organ transplantation to improve one's quality of life. Also, conditions such as diabetes and obesity can be detrimental to one's life and can lead to fatty liver disease which can lead to chronic liver disease requiring liver transplantation if the liver decompensates.
The development of organ transplantation in the second half of the 20th century has been a remarkable achievement. Recently; organ transplantation is one of the most effective options for those with an end-stage organ failure. Its success has been basically dependent on public awareness, support and active participation. Without these factors, the efficiency of organ transplantation and the consequent saving or extension of lives would have undoubtedly suffered adversely.
The number of patients in need of organ transplantation has increased at a rapid pace; in contrast, the number of available organs has increased only slightly. Expanded criteria for donor selection, such as older age, have resulted in more people who meet the criteria for brain death becoming organ donors although fewer organs are transplanted from each donor. Improvements in automobile and highway safety, as well as increased enforcement of gun control laws, have also contributed to a plateau in the number of young, healthy donors. Public education efforts that encourage organ donation may be effective in getting more people to sign organ donor cards, but most individuals who do so will never be in a position to become organ donors.
Faced with increasing numbers of patients who need transplantation, deaths on the waiting list, and a fixed number of available organs, some transplant programs are working to increase the number of transplants from living donors. Although living donation has always been an option for some types of transplants, many programs have been reluctant to promote it, as living donation requires invasive surgery on a healthy person with associated risks of morbidity and mortality. For example, since dialysis is an option for patients with end-stage renal disease, surgery on a healthy donor may be difficult to justify, despite the dialysis patient's diminished quality of life.
The most important in organ donation is to maximize the psychological status and well-being of the donors before and after transplantation has become the foremost goal of all transplantation centres. The psychological issues that mainly concern with the living organ donation includes prevention of psychological harm, ensuring the donors are fully informed and decide to donate without coercion, monitoring donor psychosocial outcomes are intimately linked to the factors that historically served as barriers to use of organs from living donors. These barriers can be overcome by the motivating of the public and creating awareness and responsibility among oneself.
Organs that can be transplanted from the living donor includes one kidney, part of intestine, pancreas, islets of Langerhans, bone, part of liver, one testis, bone marrow and blood. The organ that can be transplanted from the deceased donor are heart, kidney, pancreas, stomach, hand, skin, blood vessels, lungs, liver, intestine, testis, cornea and heart valve.
Types of organ donation
-
Autograft: Transplanting a person's tissues from one site and use it in another site of his body and is called autograft. For example, removal of skin from the legs and using it for damaged skin face or other exposed part. -
Allograft: Transplant of an organ between two genetically non identical individuals, it is called allograft. Due to the genetic difference, the donor's organ will be treated as foreign by the recipient and will try to destroy it. This is called s rejection. -
Isograft: Transplant of organ/tissue from a donor to genetically identical recipient is called isograft. There will not be any immune response hence no transplant rejection. -
Xenograft: Transplantation of organ/tissues forms one species to another species. For example, the heart valve of pig is transplanted successfully to human. -
Split transplant: An organ like liver retrieved from the deceased donor can be divided between two recipients, usually an adult and a child. -
Domino transplant: When the lungs are to be transplanted, surgically it is easier to replace them along with the heart. If the recipient's original heart is healthy, it can be transplanted into another recipient in the need of one. -
ABO incompatible transplantation: The immune system of young children aged below 12 months might have developed fully. They can receive organs from incompatible donors.
Types of donors
-
Live donors: A living person, mentally and physically healthy can donate one of a paired organ, part of an organ or a tissue. The organs donated are kidneys, part of live, one of the lung, part of small intestine, skin, bone marrow, one of the testis and one of the ovaries. Live donor can either be related or unrelated. -
Unrelated donors: For altruistic reasons, a person can donate one of his organs to an unrelated donor. According to TOHO act, the unrelated donor should be known to the recipient and have some obligation to him. It has to be established that there is no monetary transaction between them. But in many other countries, even a stranger can donate one of his organs to a needy person on altruistic grounds. -
Deceased donors: Organs are harvested from brain dead person whose respiration and circulation are maintained artificially. Brain dead has to be certified by a team of doctors nominated by Government I every organ retrieval centers. -
Paired exchange: When a living donor is not compatible with the related recipient, but may be compatible for another recipient. That second recipient related donor is compatible to the first recipient, then permission can be granted for transplantation. The surgery for all four donors and recipient are conducted simultaneously and anonymity is kept until after the transplant. -
Spousal donation: A spouse can donate an organ to the partner. It has to be recorded that the couple is legally married.
Advertisement
3. Current scenario: trends
Despite advances in medicine and technology, and increased awareness of organ donation and transplantation, the gap between supply and demand continues to widen. Each year, the number of people in the waiting list is increasing in both donor and transplant. The donation statistics according to OPTN Annual report shows that in 2016, total of 41,335 organs were donated. It can be either deceased or living and four out of five donations came from deceased donors and four out of ten from living donors. According to the report by OTPN 2018, 115,033 people need life-saving organ transplant, of those 74,926 people are the active waiting list candidates.
The real reason behind a living person's interest in donating one's organ is important to determine but it is often difficult. Now days, money has become the motivation for donation. The relationships also have played a great role in increasing donation rates. The shortage of available organs can be reduced if; people choose to donate their organs after they die. If more people did that the issue regarding organ shortage can be minimized.
The trend is expected to accelerate each year. Many organ procurement and the Joint Commission on Accreditation of Healthcare Organizations actively participate to increase the donation rates. The organizations take various to steps against traditional social taboos.
The approach, known as "donation after cardiac death" (DCD), usually involves patients who have suffered brain damage, such as from a car accident or a stroke. After family members have made the difficult decision to discontinue a ventilator or other life-sustaining treatment, organ-bank representatives talk to them about donation. Sometimes, the donor is suffering from an incurable disease also end up with the decision of organ donation.
According to U.S Department of Health and Human Services, more than 1,23,000 men, women and children currently needed life-saving organ transplants every 10 minutes and another name is added to the national organ transplant waiting list. In 2014, more than 8500 deceased donors made possible approximately 24,000 organ transplants. In addition, there were nearly 6000 transplants from living donors. In India, nationally with a population of 1.2 billion people, the statistics stands 0.08 persons as organ donor populations. Mrithasanjeevani, Kerala network of organ sharing which began in 2012, also states that the need for organ transplantation is high as the patients in waiting list is increasing day by day who requires organ transplantation.
The need for organ has gone up substantially all over the world. India also suffers from acute organ shortage with little to no solution for this issue. It is estimated that every year 1.5 lakh people suffer from renal failure out of which only 3000 people get donors. Similarly, every year around 2 lakh people die of liver failure or cancer and rarely get any help in the form of organ donors. It is the same for heart patients, for every 50,000 heart attack patients there are only 15 hearts available for transplant. Therefore, there is an urgent need for widespread campaigns to spread awareness about organ donation in India and to bridge the gap between supply and demand. The numbers that are mentioned here are estimates and real numbers could be far more than this, it is scary because this means very few people get relief and get a second chance in life.
Advertisement
4. Challenges in organ donation
As far as the challenges concerned it includes mainly donor's motives for donation, the predominant ways in which donors arrive at the decision to donate, and the donors' psychological status and its relationship to their fitness as donors.
4.1. Pre-donation challenges
4.1.1. Donor's motives
Most donors are likely to be motivated by multiple factors. These factors include intrinsic factors (e.g., desires to relieve the suffering of another or to act in according to the religious convictions) and extrinsic factors (e.g., the social pressures or perceived norms) that may operate simultaneously. The particular combination of motivational forces will also differ depending on whether and how the donor is related to the recipient.
Among living related donors, it has long been assumed that family members or emotional partners are motivated primarily for saving the lives of their loved ones. Such motives are indeed the most commonly expressed feelings, as noted in a variety of studies over the past 30 years. Among nondirected living donors (individuals donating to unrelated patients whom the donors did not select)(NDLDs), it was identified as the altruistic/humanitarian motives, along with beliefs that the donor's self-worth would be improved, and feelings of moral and religious obligation or self- identity.
4.1.2. Donor's decision-making
The motivation for the organ donation is purely on the donor's decision of organ donation and it may be influenced by many factors including the relationship to the recipients. Decision-making swiftness may indicate the type of decision being made. There appear to be two decision-making approaches that include the moral decision making and the rational decision making. "Moral decision-making" involves awareness that one's actions can affect another; ascription of responsibility to oneself; acceptance of the social/moral norm governing the behavior; and taking action consistent with that norm. Because moral decision-making does not involve the costs and benefits of a given behavior but, instead, is based on perceived norms governing that behavior, it is likely to lead to non- deliberative, instantaneous decisions. In contrast, "rational" decision-making includes various steps that focus on gathering relevant information, evaluating alternatives, selecting an alternative, and implementing the decision.
4.1.3. Support
It includes mainly the assessment of the donor's available physical, financial and emotional support. It is necessary to identify whether the donor have someone to provide care in the recovery period, have sufficient financial support and so on. This important to avoid distress if the donor develops any complications. Finally, does the donor have the support of significant others for being a donor, or is he or she choosing to donate over the objections of persons who have a legitimate interest in the outcome of an autonomous decision.
4.1.4. Family attitudes toward donation
Spouse and family attitudes about donation should also be explored. Collateral interviews with significant others is necessary, especially those who will be providing tangible support to the donor during the recovery period, should be conducted whenever possible. Conflicts between potential donors and significant others should be addressed and, ideally, resolved prior to surgery itself in order to avoid conflicts later. Family members should provide a good understanding of the donor's wishes and motives, even if they agree to disagree to the donor's decision.
4.1.5. Behavioral and psychological health
The behavioral and psychological health of the donor should also be considered before donation. It is important to identify donor's lifestyle is sufficiently healthy to reduce unnecessary risk for both donor and recipient. Many potential donors may have some unhealthy behaviors, such as moderate obesity or smoking. It is necessary to identify that there is sufficient time for the donor to reduce risks (e.g., lose weight, stop smoking). Moreover, it needs to be taken care of that the donor is emotionally stable to cope with stresses which may come up before, during, and after the donation. Hence it is important to identify psychological and behavioral status of the donor or else it may affect the quality of life.
4.1.6. Donor-recipient relationship
The relationship between the donor and recipient is a complex matter. Even when both parties are agree for donation and transplant, family dynamics may be complicated, and other family members may assertively involve themselves in the decision-making process. The donor may have unrealizable expectations that transplant will alter his or her relationship with the recipient. The health care team should not expect an ideal relationship in which all interactions between donor and recipient are harmonious. However, obvious tensions and overt psychological issues should be addressed. Joint interviews, involving both donor and recipient, should be avoided early in the evaluation process in order to preserve privacy and give the potential donor the opportunity to express reservations or "opt out" gracefully.
4.1.7. Diversity issues
Non directed donors may have diversity concerns that may affect the organ donation. The potential donors should be assessed for comfort with donation to recipients of different genders, races, religions, sexual orientations, nationalities, ages, underlying diseases, and lifestyles. Donors who express objections, fears, or concerns about who might receive their organ may need to be deferred until they can receive counseling.
4.1.8. Psychological status of potential donors
The potential donor's psychological status is of greatest concern for donation and transplantation. Concerns have been particularly high in case of unrelated donation (either directed to a specific patient, or NDLD): the willingness or desire to donate to a stranger has been historically viewed with suspicion and as likely to reflect significant psychopathology. There is no doubt that some potential donors will be psychologically poor candidates to serve as donors.
4.1.9. Post-donation challenges
The donors' perceptions of their physical functional, psychological, and social well-being were found to be either nonsignificantly different from or significantly better than levels reported in the general population. The post challenges mainly includes recipient death or graft loss, donor medical complications, donor history of mood or other psychiatric problems, and poor donor relationships with recipient or family. The other factor is that it may affect the donor's quality of life if any complication arises.
The post transplantation challenges are many which include minimizing rejection risks, immunosuppression, organ shortage, handling of the stressors of transplantation, psychosocial adaptation and psychological disorders and so on.
4.1.10. Minimizing rejection risks
The twin conditions of antibody sensitization and antibody-mediated rejection remain challenging and frustrating to treat. The recent drugs which are used to desensitize patients or reverse antibody-mediated rejection, especially chronic antibody mediated rejection is totally unsatisfactory. Development of therapies those are more effective and less toxic should be made available. Recent regimens used for antibody desensitization and reversal of antibody-mediated rejection include plasmapheresis, immunoglobulin (IVIG), and rituximab, an anti-chimeric, anti-CD20 antibody. Recently, the proteasome inhibitor Velcade has also been reported to reverse refractory antibody rejection. Eculizumab, a humanized anti-C5 monoclonal antibody appears to protect the renal allograft despite the presence of donor-specific antibodies (DSA). None of these agents have been tested in rigorous studies.
4.1.11. Immunosuppression
This is one of the major challenges after organ transplantation. Many studies have suggested that most of the late graft loss occurs because of immunologic reasons, frequently antibody-mediated. So the approach of minimizing immunosuppression is necessary with the present drugs to reduce toxicities may actually be helpful in the long-term survival of the graft. The toxicities are minimized by allowing more grafts to be rejected by immune mechanisms. Hence, development of effective agents that lack long-term toxicities so that we can maintain optimum immunosuppression over the long-term.
4.1.12. Stressors after transplantation
In the perioperative period, the focus is on the patient's physical recovery, with possible rejection episodes and other medical complications causing anxiety and emotional strain. Within the first days after transplantation, a postoperative delirium can occur. The patient can present with symptoms of mental confusion, language disturbances, and occasional hallucinations and delusions are often a frightening experience to patients and their families. Acute brain dysfunction can occur in intensive care patients and patients after surgery. The corticosteroids which are administered for immunosuppression cause these problems. Some of the patients experience problems in accepting the new organ from another individual and suffer with feeling of guilt towards the donor which, in turn, can increase psychological stress and nonadherence [6, 7, 8, 9, 10, 11].
In the long-term postoperative period, medication side effects and associated comorbidities become central stressors impeding patient's life quality. Most common comorbidities seen are infections, diabetes mellitus, hypertension, lipometabolic disorders, adipositas, cardiovascular diseases, oncological diseases, osteoporosis, and chronic kidney failure [12, 13]. Furthermore, psychiatric symptoms (e.g., depression, anxiety, agitation, psychosis) and neurological symptoms (e.g., sleep disturbances, cognitive impairment, delirium) can occur as neurotoxic side effects in patients receiving immunosuppressive drugs.
Faced with the multiple health risks, patients often continue to experience anxiety and worries regarding possible retransplantation, serious comorbidities, and death. Even patients in good physical health are confronted with severe challenges, for example, regaining their previously lost or restricted social roles as family members and partners (including sexual activity) and returning to work or taking up other meaningful activities. Financial constraints and legal disputes with health or pension insurance agencies constitute other possible sources of psychological strain.
Advertisement
5. Psychosocial adaptation and psychological disorders
After the transplantation, the psychosocial burden more severe in preoperative period than postoperative period. Nevertheless, patients themselves have to demonstrate considerable coping skills. In the best case, transplant patients learn to adapt to their new situation, often by reevaluating life goals and by focusing on more positive consequences, for example, personal growth. On the other hand, unsuccessful readjustment can lower the quality of life and psychiatric morbidity. The most common psychological disorders among patients before and after transplantation are affective and anxiety disorders.
The literature review shows that prevalence of depression in 20–25% of cases before and after kidney transplantation. Less information is available concerning patients receiving other organs. Prior to and following lung transplantation, depression seems to be prevalent in approximately 30% of patients. Hence these show that the depression is a major challenge after transplantation. These issues can be reduced by personal and social resources (resilience factors), that is, favorable coping skills, self-efficacy, sense of coherence, optimism, and social support.
Advertisement
6. Factors affecting donor's motivation
There are many factors affecting donor's motivation which includes feelings of love and responsibility, spiritual motives, and greater success rate of organ donation.
6.1. Feelings of love and responsibility
Motives for donating organ to their relative patients were that they tended to do something for their loved ones. In fact, they feel responsible for their problems. They do not treat others' problems with indifference and attempted to do whatever they could for resolving the problems experienced by transplant recipients. It is considered as their own responsibilities to help them to get rid of their problems. The feel like they are the ones who need to support their patients.
6.2. Close and constant companionship
Another factor affecting the participants' feeling of responsibility for donation to their family members was close and constant companionship with recipients. This close and constant companionship made the participants to clearly understand the recipients' conditions and hence, it had resulted in their decision on organ donation in order to alleviate recipients' problems. This close and constant companionship with patients help family members understand patients' problems well and increase their degree of commitment to do something for patient's pain and discomfort. They also noted that this had made them experience deeper shared emotions with their patients and hence, required them to feel responsible for minimizing their patient's problems.
6.3. Inability to tolerate recipient's discomfort
Another motive for organ donation was one's difficulty in tolerating recipient's discomfort. Love for their sick family members had made the participants feel responsible and decide on doing something for solving their patient's problems. Their patient's pain, suffering and discomfort cause a great inconvenience and irritation which lead them to the decision of organ donation. They hoped that organ donation alleviate their patient's problems [14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 36].
6.4. Spiritual motives for donation
Religious beliefs played a significant role in motivating to organ donation. Some of them believed that donation was a way for expiating their past sins. They referred to faith in God, reliance on Him, and hope for a successful transplant as the important motives for organ donation. Some of them even accused themselves of causing their family members to develop organ failure and believed that donation was a way for alleviating their feelings of guilt. Such a practice was particularly common among the parents of sick children. Some of them considered donation as a God-approved practice, and noted that God has helped them donate their organs. They noted that they donated their organs for gratifying God and believed that he sees it and help them in all bad situations.
6.5. Greater success rate of organ transplantation
The category is the greater success of organ transplantation. In other words, obtaining information and realizing the greater benefits of organ transplantation had motivated the participants to opt for organ donation. Some of them reported that they had never thought about donation until obtaining information from their patient's physicians. However, after obtaining adequate information, they had made an irreversible decision about organ donation. Accordingly, a major motive for organ donation was the lower likelihood of organ rejection.
Advertisement
7. Measures to overcome challenges for organ donation
The decisions regarding organ donation based on the personal beliefs (religious, cultural, family, social and body integrity) levels of knowledge about organ donation and previous interaction with the health care team. Many maintained positive attitudes to organ donation despite significant reservations about the organ donation process. Resistance to organ donation found to be less in the case of living donation for family.
There are some religious beliefs that can have both positive and negative influences, these often stemmed from uncertainty or misrepresentation of religious edicts. One solution would be to actively engage religious leaders in the transplant community, especially when it has been reported that, across the major religions, there are very few cases where organ donation can be seen to be inconsistent with religious beliefs. Religious leaders should be made available in hospitals and other transplantation setting to assist families in making decisions regarding organ donation and potentially to remove the misperceptions. Staff members who are involved in approaching families to request consent for donation should be part of the awareness programs and resources about religious concerns. Similarly, cultural sensitivity to issues such as apprehensiveness to discuss death among certain groups or individuals and the importance to many of death rituals may improve dialog regarding organ donation.
Studies have shown that engaging some minority groups in the health care system and creating a sense of belonging and ownership can improve compliance with organ donation. As a consequence, more efforts should be made to create positive interactions within the health care team members, especially for minority groups, to improve the organ donation rates. Although many of the studies have showed that higher socio-economic status and education were associated with a stronger willingness to be an organ donor. Some of the strong reservations held, even among those with generally positive views towards donation, such as concerns that agreeing to donation would discourage doctors from caring so much about saving their lives in case of an emergency or that it would result in the premature removal of their organs or indeed prevent them from having an open coffin at their funerals, are examples of very real barriers that can be readily addressed through information. Through a proper awareness and motivation the donation rates can be improved which can save many lives.
7.1. Psychological care
Psychological consultation is essential for all disease stages enabling patients to better cope with their extraordinarily stressful situation. A need for psychological care was found in up to 50% of transplant patients. Educational and supportive therapies are of utmost importance but also cognitive-behavioral interventions including relaxation techniques can also be considered. Less common methods like hypnotherapy and "Quality of Life Therapy" have also been utilized for overcoming the challenges.
Moreover, family members as well as caregivers of transplant patients show increased psychological strain before and after transplantation. Family counseling, and psychotherapeutic support, can help reduce psychological strain, thus also maintaining the valuable social support provided by care givers and family members of the transplant patient. Henceforth, the family and care givers should also be considered in psychosocial evaluation to overcome the problems.
7.2. Alternative methods to increase donation
In view of ethical, legal and political issues, it was deemed important to obtain some opinion about alternative methods to increase organ donation rates. Financial incentives were given to increase organ donation. Many in both donor and non-donor groups were given a reasonable incentive. Education and dissemination of information about donation and transplantation was important to increase organ donation rates. There was nearly universal agreement that implied consent (presumed consent) should not be tried. The use of financial incentives was not markedly opposed (some accepted the idea of funeral expense reimbursement), although there was not strong support either. In general, methods to increase organ donation had not been well thought out by either donors or nondonors indicating, perhaps, that the assumption of altruism or motivation is the best way to increase the donation rates.
Advertisement
8. Responsibilities of nurses in organ donation and transplantation
Organ and tissue transplant nurses need comprehensive and scientific knowledge. They include the evaluation and management of deceased donors, transplant recipients, potential donors or live donors, teaching and counseling of transplant recipients and live donors related to self-care management, healthy life and a peaceful death when this is imminent. This is important in order to improve the posttransplant quality of life.
Nurses have important role in the development of a successful transplantation program. They are key members of the team that works to deliver care to patients and relatives, through the use of technological, logistic and human resources, with a view to coordination, care, education and research on organ and tissue donation and transplantation. Therefore, the nurses need adequate knowledge on the principles of good ethical principles and should have resources available for them to assess patient's risks and social issues related to organ transplants and donation. The researchers hope that the future studies will encourage further researches on the role and responsibilities of nurses.
Advertisement
9. Conclusion
The organ donation decision is a complex one, based strongly on personal beliefs. There are some factors, such as religious and cultural beliefs, that are seemingly intractable and are often cited as reasons for a refusal to donate. In this chapter, it is shown that these have often been found to be tied in with more complex issues such as a distrust of the medical system, misunderstandings about religious stances and ignorance about the donation process. Interventions to better engage the community, including disadvantaged and minority groups, to foster trust and provide information represent promising opportunities of promoting organ donation in the future.
Donor motives directly contribute to their decision to donate, is not uniform and is influenced by multiple factors. Majority of the donors were relationship oriented donor, whose major motives were desires to relieve the suffering & save the life of their loving ones. Creating awareness to the organ donation will directly influence the donor motives and willingness. By deriving the motives many more intervention to improve the willingness to be a living organ donor can be evolved. Recruitment of living donors represents a medical and moral responsibility. The possibility of organ removal from healthy donor to a recipient needs great inner motivation. Saving one's life is divine.
The psycho social assessment must be made as a routine part of the nursing process. These assessments are meant to identify patients at risk for poor outcomes, provide guidelines for their management and improve the post-transplant quality of life [6]. "Because donated organs are a severely limited resource, the best potential, recipients should be identified. The probability of a good outcome must be highly emphasized to achieve the maximum benefit for all transplants" (OPTN/UNOS Ethics committee General Considerations in Assessment for Transplant Candidacy White paper-2010).
References
- 1.
United Network for Organ Sharing. 1999 Annual Report of the U. S. Scientific Registry of Transplant Recipients and the Organ Procurement and Transplantation Network.: Transplant Data 1989–1998. Richmond, Va: US Department of Health and Human Services, Health Research Services Administration, Office of Sponsored Projects, Division of Transportation, and United Network for Organ Sharing; 2000 - 2.
Alexander JW, Zola JC. Expanding the donor pool: Use of marginal donors for solid organ transplantation. Clinical Transplantation. 1996; 10 :1-19 - 3.
Kumar A, Mandhani A, Verma BS, et al. Expanding the living related donor pool in renal transplantation: Use of marginal donors. Journal of Urology. 2000a; 163 :33-36 - 4.
Mandal AK, Kalligonis AN, Ratner LE. Expanded criteria donors: Attempts to increase the renal donor transplant pool. Advances in Renal Replacement Therapy. 2000a; 7 :117-113 - 5.
Simmons RG et al. Gift of Life: The Social and Psychological Impact of Organ Transplantation. NY: Wiley; 1977. Reprinted with additions, Brunswick, NJ: Transaction Books, 1987 - 6.
Corley MC et al. Attitude, self-image, and quality of life of living kidney donors. Nephrology Nursing Journal. 2000; 27 (1):43-52 - 7.
Goldman LS. Liver transplantation using living donors: Preliminary donor psychiatric outcomes. Psychsomatics. 1993; 34 (3):235-240 - 8.
Pradel FG et al. Exploring donors' and recipients' attitudes about living donor kidney transplantation. Progress in Transplantation. 2003; 13 (3):203-210 - 9.
Fellner CH. Renal transplantation and the living donor. Decision and consequences. Psychother Psychosomat. 1976/77; 27 :139-143 - 10.
Toronyi E et al. Attitudes of donors towards organ transplantation in living related kidney transplantations. Transplant International. 1998; 11 (Suppl 1):S481-S483 - 11.
Henderson AJZ et al. The living anonymous kidney donor: Lunatic or saint? American Journal of Transplantation. 2003; 3 :203-213 - 12.
Jacobs CL et al. Twenty-two nondirected kidney donors: An update on a single center's experience. American Journal of Transplantation. 2004; 4 :1110-1116 - 13.
Matas AJ et al. Nondirected donation of kidneys from living donors. The New England Journal of Medicine. 2000; 343 (6):433-436 - 14.
Olbrisch ME et al. Psychological, Social and Behavioral Characteristics of Living Donor Candidates for Adult Liver Transplantation. Biennial Meeting on Psychiatric, Psychosocial and Ethical Issues in Organ Transplantation. Santa Monica, CA; February, 2005 - 15.
Crowley-Matoka M et al. Long-term quality of life issues among adult-to-pediatric living donors: A qualitative exploration. American Journal of Transplantation. 2004; 4 :744-750 - 16.
Karliova M et al. Living-related liver transplantation from the view of the donor: A 1-year follow-up survey. Transplantation. 2002; 73 (11):1799-1804 - 17.
De Graaf Olson W, Bogetti-Dumlao A. Living donors' perception of their quality of health after donation. Progress in Transplantation. 2001; 11 (2):108-115 - 18.
Beavers KL et al. The living donor experience: Donor health assessment and outcomes after living donor liver transplantation. Liver Transplant. 2001; 7 (11):943-947 - 19.
Lennerling A et al. Becoming a living kidney donor. Transplantation. 2003; 76 :1243-1247 - 20.
Pradel FG. Exploring donor's and receipient's attitudes about living door kidney transplantation. Progress in Transplantation. 2003; 13 (3):203-210 - 21.
Smith MD. Living related kidney donors. A multicenter study of donor education, socioeconomic adjustment and rehabilitation. American Journal of Kidney Diseases. 1986; 8 (4):223-233 - 22.
Jacobs CL. Expanding living donor options. Minnesota Medicine. 2001; 84 :46-48 - 23.
Switzer GE. Understaning donor;s motivations. A study of unrelated bone arrow donors. Social Science & Medicine. 1999; 45 (1):137-147 - 24.
Rosenthal JT. Expanded criteria for cadaver organ donation in renal transplant. The Urologic Clinics of North America. 1994; 21 :283-292 - 25.
Shiel AGR. Transplantation and society. In: Ginns LC, Cosimi A, Morris PJ, editors. Transplantation. Malden, MA: Blackwell Science; 1999. pp. 897-913 - 26.
Callender CO, Bay AS, Miles PV, Yeager CL. A national minority organ/tissue transplant education program: The first step in the evolution of a national minority strategy and minority transplant equity in the USA. Transplantation Proceedings. 1995; 27 :1441-1443 - 27.
Surman OS et al. Live organ donation: Social context, clinical encounter, and the psychology of communication. Psychosomatics. 2005; 46 :1-6 - 28.
Papachristou C et al. Motivation for living-donor liver transplantation from the donor's perspective: An in-depth qualitative research study. Transplantation. 2004; 78 :1506-1514 - 29.
Haljamäe U. Remaining experiences of living kidney donors more than 3 yr after early recipient graft loss. Clinical Transplantation. 2003; 17 :503-510 - 30.
Hamburger J, Crosnier J. Moral and ethical problems in transplantation. Rapaport F, Daussert J. Human Transplantation. NY: Grune & Stratton; 1968. pp. 68 - 31.
Sadler HH et al. The living, genetically unrelated, kidney donor. Seminars in Psychiatry. 1971; 3 :86-101 - 32.
Walter M et al. Psychosocial outcome of living donors after living donor liver transplantation: A pilot study. Clinical Transplantation. 2002; 16 :339-344 - 33.
Fukunishi I et al. Psychiatric disorders before and after living-related transplantation. Psychosomatics. 2001; 42 (4):337-343 - 34.
Crowley-Matoka M, Switzer G. Nondirected living donation: A survey of current trends and practices. Transplantation. 2005; 79 (5):515-519 - 35.
Boparai J, Davila H, Chandalia M. Cardiovascular disease in Asian Indians living in the United States. Current Cardiovascular Risk Reports. 2011; 5 :240-245 - 36.
Ji WR, Frederick B, Hsin CY. Trends in prevalence of Type 2 diabetes in Asians Versus Whites results from the United States National Health Interview Survey 1997-2008. Diabetes Care. Feb 2011; 34 (2):353-357
Submitted: November 13th, 2017 Reviewed: April 3rd, 2018 Published: July 25th, 2018
© 2018 The Author(s). Licensee IntechOpen. This chapter is distributed under the terms of the Creative Commons Attribution 3.0 License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
edwardsworgalenly.blogspot.com
Source: https://www.intechopen.com/chapters/62192
0 Response to "Do Organs Continue to Grow After Theyve Been Donated"
Postar um comentário